
HbA1c, or glycated hemoglobin, is a measure of average blood glucose over a period of a few months. Blood glucose glycates (i.e., sticks to) hemoglobin, a protein found in red blood cells. Red blood cells are relatively long-lived, lasting approximately 3 months. Thus HbA1c (given in percentages) is a good indicator of average blood glucose levels, if you don’t suffer from anemia or a few other blood abnormalities.
Based on HbA1c, one can then estimate his or her average blood glucose level for the previous 3 months or so before the test, using one of the following equations, depending on whether the measurement is in mg/dl or mmol/l.
Average blood glucose (mg/dl) = 28.7 × HbA1c − 46.7
Average blood glucose (mmol/l) = 1.59 × HbA1c − 2.59
Elevated blood glucose levels cause damage in the body primarily through glycation, which leads to the formation of advanced glycation endproducts (AGEs). Given this, HbA1c can be seen as a proxy for the level of damage done by elevated blood glucose levels to various body tissues. This damage occurs over time; often after many years of high blood glucose levels. It includes kidney damage, neurological damage, cardiovascular damage, and damage to the retina.
Most regular blood exams focus on fasting blood glucose as a measure of glucose metabolism status. Many medical practitioners have as a target a fasting blood glucose level of 125 mg/dl (7 mmol/l) or less, and largely disregard postprandial glucose levels or HbA1c in their management of glucose metabolism. Leiter and colleagues (2005; full reference at the end of this post) showed that this focus on fasting blood glucose is a mistake. They are not alone; many others made this point, including some very knowledgeable bloggers who focus on diabetes (see “Interesting links” section of this blog). Leiter and colleagues (2005) also provided some interesting graphs and figures, including eye-opening correlations between various variables and arterial stiffness. The figure below (click to enlarge) shows the contribution of postprandial glucose to HbA1c.

Note that the lower the HbA1c is in the figure (horizontal axis), the higher is the postprandial glucose contribution to HbA1c. And, the lower the HbA1c, the closer the individuals are to what one could consider having a perfectly normal HbA1c level (around 5 percent). That is, only for individuals whose HbA1c levels are very high, fasting blood glucose levels are relatively reliable measures of the tissue damage done be elevated blood glucose levels.
The table below (click to enlarge) shows P values associated with the impact of various variables (listed on the leftmost column) on arterial stiffness. This measure, arterial stiffness, is strongly associated with an increased risk of cardiovascular events. Look at the middle column showing P values adjusted for age and height. The lower the P value, the more a variable affects arterial stiffness. The variable with the lowest P value by far is 2-hour postprandial blood glucose; the blood glucose levels measured 2 hours after meals.
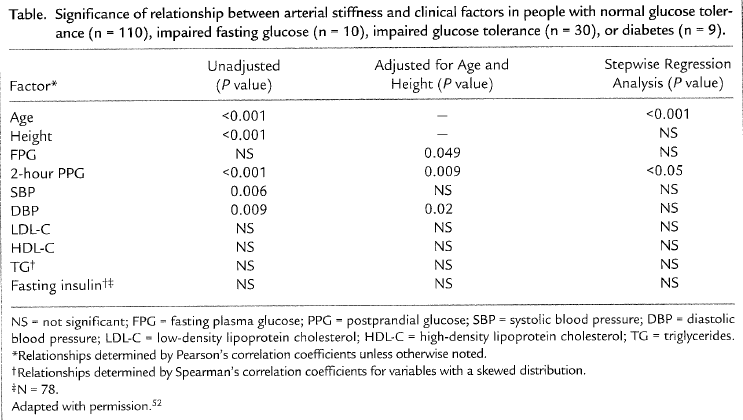
Fasting glucose levels were reported to be statistically insignificant because of the P = 0.049, in terms of their effect on arterial stiffness, but this P value is actually significant, although barely, at the 0.05 level (95 percent confidence). Interestingly, the following measures are not even on the radar screen, as far as arterial stiffness is concerned: systolic blood pressure, LDL cholesterol, HDL cholesterol, triglycerides, and fasting insulin levels.
What about the lipid hypothesis, and the “bad” LDL cholesterol!? This study is telling us that these are not very relevant for arterial stiffness when we control for the effect of blood glucose measures. Not even fasting insulin levels matters much! Wait, not even HDL!!! A high HDL has been definitely shown to be protective, but when we look at the relative magnitude of various effects, the story is a bit different. A high HDL’s protective effect exists, but it is dwarfed by the negative effect of high blood glucose levels, especially after meals, in the context of cardiovascular disease.
What all this points at is what we could call a postprandial glucose hypothesis: Lower your postprandial glucose levels, and live a longer, healthier life! And, by the way, if your postprandial glucose levels are under control, lipids do not matter much! Or maybe your lipids will fall into place, without any need for statin drugs, after your postprandial glucose levels are under control. One way or another, the outcome will be a positive one. That is what the data from this study is telling us.
How do you lower your postprandial glucose levels?
A good way to start is to remove foods rich in refined carbohydrates and sugars from your diet. Almost all of these are foods engineered by humans with the goal of being addictive; they usually come in boxes and brightly colored plastic wraps. They are not hard to miss. They are typically in the central aisles of supermarkets. The sooner you remove them from your diet, the better. The more completely you do this, the better.
Note that the evidence discussed in this post is in connection with blood glucose levels, not glucose metabolism per se. If you have impaired glucose metabolism (e.g., diabetes type 2), you can still avoid a lot of problems if you effectively control your blood glucose levels. You may have to be a bit more aggressive, adding low carbohydrate dieting (as in the Atkins or Optimal diets) to the removal of refined carbohydrates and sugars from your diet; the latter is in many ways similar to adopting a Paleolithic diet. You may have to take some drugs, such as Metformin (a.k.a. Glucophage). But you are certainly not doomed if you are diabetic.
Reference:
Leiter, L.A., Ceriello, A., Davidson, J.A., Hanefeld, M., Monnier, L., Owens, D.R., Tajima, N., & Tuomilehto, J. (2005). Postprandial glucose regulation: New data and new implications. Clinical Therapeutics, 27(2), S42-S56.
Good stuff Ed though I would suggest that the highness of morning post prandials has a lot to do with the release of counterregulatory hormones that essentially make you more insulin resistant in the mornings.
ReplyDeleteDiabetics have been hyping post prandials for awhile. We, however, frequently use the 1 hour time limit to evaluate food spikes.
This brings me to the question of time. The biggest question I have is, how long must the post prandials be elevated before there is significant glycation? This is the one study I have not been able to find.
I had something on that, from a study that looked at longitudinal data on both glucose variations and HbA1c. Not ideal but close. I wish I had stored it, because I cannot find it now.
ReplyDeleteFrom what I recall, area under the curve (AUC) was the key, but this effect was confounded by the degree of elevation. (Someone can have a higher AUC, and lower elevations; a somewhat controlled diabetic vs. a careless but normoglycemic eater of high-carb foods.) There was another issue at play. Some people seem deal with glycation better than others, and one postulated mechanism was more intense autophagy.
My speculation is that low carb dieting, intermittent fasting, and even just having low body fat, all increase the rates of autophagy.
I need to find that paper.
"Some people seem deal with glycation better than others, and one postulated mechanism was more intense autophagy."
ReplyDeleteHow does this jibe with Jenny Ruhl's idea that her A1c numbers stay relatively high because she believes that her blood cells are longer lived and therefore the A1c is actually measuring a longer period of glycation.
Hi Michael.
ReplyDeleteIf I recall it correctly from her site, her HbA1c is 5.8% or so. If yes, it is not bad at all. And based on the study reviewed in this post, she is doing the absolutely right thing controlling her postprandial sugars with diet and (if I am not mistaken) exogenous insulin.
I think autophagy is related to apoptosis, and may even influence it to a certain extent. I think apoptosis in red blood cells is called eryptosis.
It makes sense to think that red blood cell lifespan varies from person to person. So many things vary in normal or quasi-normal way in any population of individuals.
This is also consistent with the wide range of possible average blood glucose levels associated with a given HbA1c. For example, an HbA1c of 5% may mean an average blood glucose in the range of 76 to 120:
http://healthcorrelator.blogspot.com/2010/04/blood-glucose-control-before-age-55-may.html
HbA1c is a good measure, I think, relative to the individual for which the measure is calculated. If person A's HbA1c is going up, then something is wrong. But HbA1c seems like an fairly imprecise measure if you want to compare different individuals.
In this context, an HbA1c of 5.8% may be pretty good. It should go up with age, but if it goes up very slowly with age, that is a positive sign.
Maybe I should have explained myself better. Ruhl's bg's through out her day average out to where her A1c should be around 5 but her A1c is about 5.8. She attributes this difference to her blood cells having a longer life than usual. Since she is very well controlled, meaning no large bg fluctuations, this would seem to be at odds with the idea of increased rates of autophagy being the agent for handling glycation.
ReplyDeleteBy the way, I remember that paper and I can understand why you didn't save it. I don't remember the particulars but I didn't find its conclusions all that useful.
One factor to consider here is that glycation is more of a function of a weighted average BG, than of an average BG. The reason is that glycation becomes more intense at elevated BGs.
ReplyDeleteThe equation that gives average BG as a function of HbA1c takes that weighted average idea into consideration, I believe.
So, using the equation to go the other way around, namely to calculate HbA1c based on measured average BG (not weighted average BG), would give an HbA1c that is slightly underestimated, I think.
As for autophagy, I think it is related to apoptosis, but it is not apoptosis (eryptosis, red blood cells is called). Autophagy is an intracellular clean-up process, which may or may not lead to cell suicide (apoptosis).
So, I can see someone having enhanced autophagy, even if that person has a tendency to have very long-lived red blood cells. The combined effect may lead to a higher HbA1c. But it can lead to a lower HbA1c too. I can't say.
When we see such a huge range of variation associated with a measure, like average BG based on HbA1c, it is usually because the measure depends on a number of factors, which are not captured by the equation.
I assume the two hour postprandial glucose reflected in your table above is the result of a clinical test based on a glucose load. In general, people who eat low carb diets will have much higher 2 hour ppg to the same glucose load as people who eat high carb diets (even though the former will have higher hdl and lower ldl). So the table seems to support a high carb diet.
ReplyDeleteHi anon.
ReplyDeleteThe numbers are based on 2-h postprandial levels measured for a sample of individuals eating their normal diet.
Given that, the table actually supports a low carb diet, or at least a low glycemic load diet, because these diets will lead to modest 2-h postprandial levels.
If the numbers were based on a controlled glucose tolerance test, then your conclusion would be correct. Congrats on being this perceptive; many people aren't.
Indeed, low carbers do become more sensitive to carbs, which is often reflected in higher glucose responses than they would normally have. Still, they reap the benefits in the long term by controlling the levels of glycation their body has to cope with.
On youtr statemnte "low carbers do become more sensitive to carbs, which is often reflected in higher glucose responses than they would normally have.". This is not necessarily true. A lot of subjects with decreased insulin sensitivity who go low carb improve their insulin sensitivity after a few months, and may show an excellent insulin response to carb load with just a small spike in BG.
ReplyDelete