
Type 2 diabetes and the “tired pancreas” theory
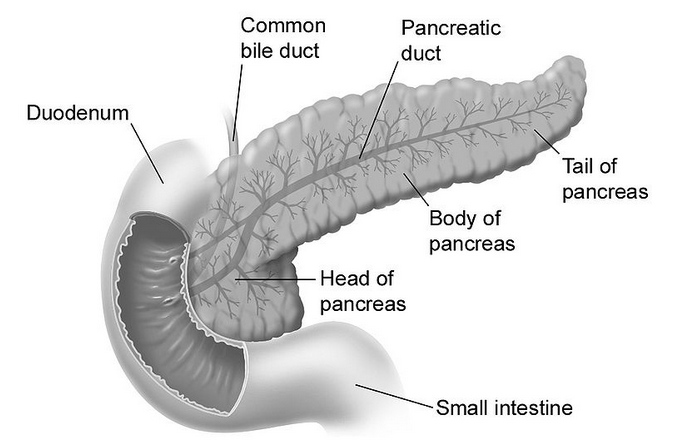
Type 2 diabetes is the one most commonly associated with the metabolic syndrome, which is characterized by middle-age central obesity, and the “diseases of civilization” brought up by Neolithic inventions. Evidence is mounting that a Neolithic diet and lifestyle play a key role in the development of the metabolic syndrome. In terms of diet, major suspects are engineered foods rich in refined carbohydrates and refined sugars. In this context, one widely touted idea is that the constant insulin spikes caused by consumption of those foods lead the pancreas (figure below from Wikipedia) to get “tired” over time, losing its ability to produce insulin. The onset of insulin resistance mediates this effect.
Empirical evidence against the “tired pancreas” theory
This “tired pancreas” theory, which refers primarily to the insulin-secreting beta-cells in the pancreas, conflicts with a lot of empirical evidence. It is inconsistent with the existence of isolated semi/full hunter-gatherer groups (e.g., the Kitavans) that consume large amounts of natural (i.e., unrefined) foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. These groups are nevertheless generally free from type 2 diabetes. The “tired pancreas” theory conflicts with the existence of isolated groups in China and Japan (e.g., the Okinawans) whose diets also include a large proportion of natural foods rich in easily digestible carbohydrates, which cause insulin spikes. Yet these groups are generally free from type 2 diabetes.
Humboldt (1995), in his personal narrative of his journey to the “equinoctial regions of the new continent”, states on page 121 about the natives as a group that: "… between twenty and fifty years old, age is not indicated by wrinkling skin, white hair or body decrepitude [among natives]. When you enter a hut is hard to differentiate a father from son …" A large proportion of these natives’ diets included plenty of natural foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. Still, there was no sign of any condition that would suggest a prevalence of type 2 diabetes among them.
At this point it is important to note that the insulin spikes caused by natural carbohydrate-rich foods are much less pronounced than the ones caused by refined carbohydrate-rich foods. The reason is that there is a huge gap between the glycemic loads of natural and refined carbohydrate-rich foods, even though the glycemic indices may be quite similar in some cases. Natural carbohydrate-rich foods are not made mostly of carbohydrates. Even an Irish (or white) potato is 75 percent water.
More insulin may lead to abnormal fat metabolism in sedentary people
The more pronounced spikes may lead to abnormal fat metabolism because more body fat is force-stored than it would have been with the less pronounced spikes, and stored body fat is not released just as promptly as it should be to fuel muscle contractions and other metabolic processes. Typically this effect is a minor one on a daily basis, but adds up over time, leading to fairly unnatural patterns of fat metabolism in the long run. This is particularly true for those who lead sedentary lifestyles. As for obesity, nobody gets obese in one day. So the key problem with the more pronounced spikes may not be that the pancreas is getting “tired”, but that body fat metabolism is not normal, which in turn leads to abnormally high or low levels of important body fat-derived hormones (e.g., high levels of leptin and low levels of adiponectin).
One common characteristic of the groups mentioned above is absence of obesity, even though food is abundant and often physical activity is moderate to low. Repeat for emphasis: “… even though food is abundant and often physical activity is moderate to low”. Note that having low levels of activity is not the same as spending the whole day sitting down in a comfortable chair working on a computer. Obviously caloric intake and level of activity among these groups were/are not at the levels that would lead to obesity. How could that be possible? See this post for a possible explanation.
Excessive body fat gain, lipotoxicity, and type 2 diabetes
There are a few theories that implicate the interaction of abnormal fat metabolism with other factors (e.g., genetic factors) in the development of type 2 diabetes. Empirical evidence suggests that this is a reasonable direction of causality. One of these theories is the theory of lipotoxicity.
Several articles have discussed the theory of lipotoxicity. The article by Unger & Zhou (2001) is a widely cited one. The theory seems to be widely based on the comparative study of various genotypes found in rats. Nevertheless, there is mounting evidence suggesting that the underlying mechanisms may be similar in humans. In a nutshell, this theory proposes the following steps in the development of type 2 diabetes:
(1) Abnormal fat mass gain leads to an abnormal increase in fat-derived hormones, of which leptin is singled out by the theory. Some people seem to be more susceptible than others in this respect, with lower triggering thresholds of fat mass gain. (What leads to exaggerated fat mass gains? The theory does not go into much detail here, but empirical evidence from other studies suggests that major culprits are refined grains and seeds, as well as refined sugars; other major culprits seem to be trans fats, and vegetable oils rich in linoleic acid.)
(2) Resistance to fat-derived hormones sets in. Again, leptin resistance is singled out as the key here. (This is a bit simplistic. Other fat-derived hormones, like adiponectin, seem to clearly interact with leptin.) Since leptin regulates fatty acid metabolism, the theory argues, leptin resistance is hypothesized to impair fatty acid metabolism.
(3) Impaired fat metabolism causes fatty acids to “spill over” to tissues other than fat cells, and also causes an abnormal increase in a substance called ceramide in those tissues. These include tissues in the pancreas that house beta-cells, which secrete insulin. In short, body fat should be stored in fat cells (adipocytes), not outside them.
(4) Initially fatty acid “spill over” to beta-cells enlarges them and makes them become overactive, leading to excessive insulin production in response to carbohydrate-rich foods, and also to insulin resistance. This is the pre-diabetic phase where hypoglycemic episodes happen a few hours following the consumption of carbohydrate-rich foods. Once this stage is reached, several natural carbohydrate-rich foods also become a problem (e.g., potatoes and bananas), in addition to refined carbohydrate-rich foods.
(5) Abnormal levels of ceramide induce beta-cell apoptosis in the pancreas. This is essentially “death by suicide” of beta cells in the pancreas. What follows is full-blown type 2 diabetes. Insulin production is impaired, leading to very elevated blood glucose levels following the consumption of carbohydrate-rich foods, even if they are unprocessed.
It is widely known that type 2 diabetics have impaired glucose metabolism. What is not so widely known is that usually they also have impaired fatty acid metabolism. For example, consumption of the same fatty meal is likely to lead to significantly more elevated triglyceride levels in type 2 diabetics than non-diabetics, after several hours. This is consistent with the notion that leptin resistance precedes type 2 diabetes, and inconsistent with the “tired pancreas” theory.
Weak and strong points of the theory of lipotoxicity
A weakness of the theory of lipotoxicity is its strong lipophobic tone; at least in the articles that I have read. There is ample evidence that eating a lot of the ultra-demonized saturated fat, per se, is not what makes people obese or type 2 diabetic. Yet overconsumption of trans fats and vegetable oils rich in linoleic acid does seem to be linked with obesity and type 2 diabetes. (So does the consumption of refined grains and seeds, and refined sugars.) The theory of lipotoxicity does not seem to make these distinctions.
In defense of the theory of lipotoxicity, it does not argue that there cannot be thin diabetics. Many type 1 diabetics are thin. Type 2 diabetics can also be thin, although this is much less common. In certain individuals, the threshold of body fat gain that will precipitate lipotoxicity may be quite low. In others, the same amount of body fat gain (or more) may in fact increase their insulin sensitivity under certain circumstances – e.g., when growth hormone levels are abnormally low.
Autoimmune disorders, perhaps induced by environmental toxins, or toxins found in certain refined foods, may cause the immune system to attack the beta-cells in the pancreas. This may lead to type 1 diabetes if all beta cells are destroyed, or something that can easily be diagnosed as type 2 (or type 1.5) diabetes if only a portion of the cells are destroyed, in a way that does not involve lipotoxicity.
Nor does the theory of lipotoxicity predict that all those who become obese will develop type 2 diabetes. It only suggests that the probability will go up, particularly if other factors are present (e.g., genetic propensity). There are many people who are obese during most of their adult lives and never develop type 2 diabetes. On the other hand, some groups, like Hispanics, tend to develop type 2 diabetes more easily (often even before they reach the obese level). One only has to visit the South Texas region near the Rio Grande border to see this first hand.
What the theory proposes is a new way of understanding the development of type 2 diabetes; a way that seems to make more sense than the “tired pancreas” theory. The theory of lipitoxicity may not be entirely correct. For example, there may be other mechanisms associated with abnormal fat metabolism and consumption of Neolithic foods that cause beta-cell “suicide”, and that have nothing to do with lipotoxicity as proposed by the theory. (At least one fat-derived hormone, tumor necrosis factor-alpha, is associated with abnormal cell apoptosis when abnormally elevated. Levels of this hormone go up immediately after a meal rich in refined carbohydrates.) But the link that it proposes between obesity and type 2 diabetes seems to be right on target.
Implications and thoughts
Some implications and thoughts based on the discussion above are the following. Some are extrapolations based on the discussion in this post combined with those in other posts. At the time of this writing, there were hundreds of posts on this blog, in addition to many comments stemming from over 2.5 million page views. See under "Labels" at the bottom-right area of this blog for a summary of topics addressed. It is hard to ignore things that were brought to light in previous posts.
- Let us start with a big one: Avoiding natural carbohydrate-rich foods in the absence of compromised glucose metabolism is unnecessary. Those foods do not “tire” the pancreas significantly more than protein-rich foods do. While carbohydrates are not essential macronutrients, protein is. In the absence of carbohydrates, protein will be used by the body to produce glucose to supply the needs of the brain and red blood cells. Protein elicits an insulin response that is comparable to that of natural carbohydrate-rich foods on a gram-adjusted basis (but significantly lower than that of refined carbohydrate-rich foods, like doughnuts and bagels). Usually protein does not lead to a measurable glucose response because glucagon is secreted together with insulin in response to ingestion of protein, preventing hypoglycemia.
- Abnormal fat gain should be used as a general measure of one’s likelihood of being “headed south” in terms of health. The “fitness” level for men and women shown on the table in this post seem like good targets for body fat percentage. The problem here, of course, is that this is not as easy as it sounds. Attempts at getting lean can lead to poor nutrition and/or starvation. These may make matters worse in some cases, leading to hormonal imbalances and uncontrollable hunger, which will eventually lead to obesity. Poor nutrition may also depress the immune system, making one susceptible to a viral or bacterial infection that may end up leading to beta-cell destruction and diabetes. A better approach is to place emphasis on eating a variety of natural foods, which are nutritious and satiating, and avoiding refined ones, which are often addictive “empty calories”. Generally fat loss should be slow to be healthy and sustainable.
- Finally, if glucose metabolism is compromised, one should avoid any foods in quantities that cause an abnormally elevated glucose or insulin response. All one needs is an inexpensive glucose meter to find out what those foods are. The following are indications of abnormally elevated glucose and insulin responses, respectively: an abnormally high glucose level 1 hour after a meal (postprandial hyperglycemia); and an abnormally low glucose level 2 to 4 hours after a meal (reactive hypoglycemia). What is abnormally high or low? Take a look at the peaks and troughs shown on the graph in this post; they should give you an idea. Some insulin resistant people using glucose meters will probably realize that they can still eat several natural carbohydrate-rich foods, but in small quantities, because those foods usually have a low glycemic load (even if their glycemic index is high).
Lucy was a vegetarian and Sapiens an omnivore. We apparently have not evolved to be pure carnivores, even though we can be if the circumstances require. But we absolutely have not evolved to eat many of the refined and industrialized foods available today, not even the ones marketed as “healthy”. Those foods do not make our pancreas “tired”. Among other things, they “mess up” fat metabolism, which may lead to type 2 diabetes through a complex process involving hormones secreted by body fat.
References
Humboldt, A.V. (1995). Personal narrative of a journey to the equinoctial regions of the new continent. New York, NY: Penguin Books.
Unger, R.H., & Zhou, Y.-T. (2001). Lipotoxicity of beta-cells in obesity and in other causes of fatty acid spillover. Diabetes, 50(1), S118-S121.
