
Type 2 diabetes and the “tired pancreas” theory
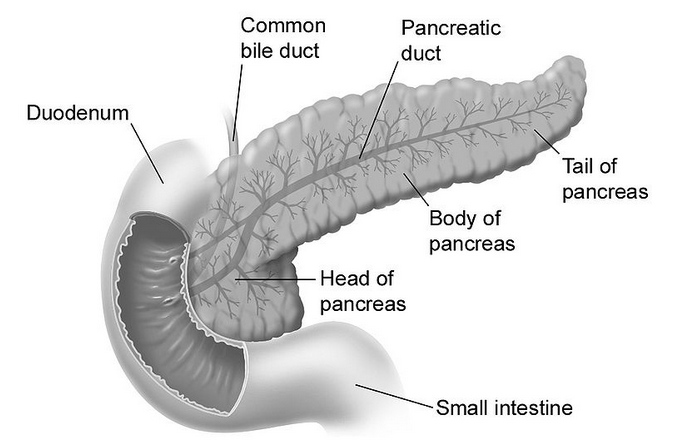
Type 2 diabetes is the one most commonly associated with the metabolic syndrome, which is characterized by middle-age central obesity, and the “diseases of civilization” brought up by Neolithic inventions. Evidence is mounting that a Neolithic diet and lifestyle play a key role in the development of the metabolic syndrome. In terms of diet, major suspects are engineered foods rich in refined carbohydrates and refined sugars. In this context, one widely touted idea is that the constant insulin spikes caused by consumption of those foods lead the pancreas (figure below from Wikipedia) to get “tired” over time, losing its ability to produce insulin. The onset of insulin resistance mediates this effect.
Empirical evidence against the “tired pancreas” theory
This “tired pancreas” theory, which refers primarily to the insulin-secreting beta-cells in the pancreas, conflicts with a lot of empirical evidence. It is inconsistent with the existence of isolated semi/full hunter-gatherer groups (e.g., the Kitavans) that consume large amounts of natural (i.e., unrefined) foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. These groups are nevertheless generally free from type 2 diabetes. The “tired pancreas” theory conflicts with the existence of isolated groups in China and Japan (e.g., the Okinawans) whose diets also include a large proportion of natural foods rich in easily digestible carbohydrates, which cause insulin spikes. Yet these groups are generally free from type 2 diabetes.
Humboldt (1995), in his personal narrative of his journey to the “equinoctial regions of the new continent”, states on page 121 about the natives as a group that: "… between twenty and fifty years old, age is not indicated by wrinkling skin, white hair or body decrepitude [among natives]. When you enter a hut is hard to differentiate a father from son …" A large proportion of these natives’ diets included plenty of natural foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. Still, there was no sign of any condition that would suggest a prevalence of type 2 diabetes among them.
At this point it is important to note that the insulin spikes caused by natural carbohydrate-rich foods are much less pronounced than the ones caused by refined carbohydrate-rich foods. The reason is that there is a huge gap between the glycemic loads of natural and refined carbohydrate-rich foods, even though the glycemic indices may be quite similar in some cases. Natural carbohydrate-rich foods are not made mostly of carbohydrates. Even an Irish (or white) potato is 75 percent water.
More insulin may lead to abnormal fat metabolism in sedentary people
The more pronounced spikes may lead to abnormal fat metabolism because more body fat is force-stored than it would have been with the less pronounced spikes, and stored body fat is not released just as promptly as it should be to fuel muscle contractions and other metabolic processes. Typically this effect is a minor one on a daily basis, but adds up over time, leading to fairly unnatural patterns of fat metabolism in the long run. This is particularly true for those who lead sedentary lifestyles. As for obesity, nobody gets obese in one day. So the key problem with the more pronounced spikes may not be that the pancreas is getting “tired”, but that body fat metabolism is not normal, which in turn leads to abnormally high or low levels of important body fat-derived hormones (e.g., high levels of leptin and low levels of adiponectin).
One common characteristic of the groups mentioned above is absence of obesity, even though food is abundant and often physical activity is moderate to low. Repeat for emphasis: “… even though food is abundant and often physical activity is moderate to low”. Note that having low levels of activity is not the same as spending the whole day sitting down in a comfortable chair working on a computer. Obviously caloric intake and level of activity among these groups were/are not at the levels that would lead to obesity. How could that be possible? See this post for a possible explanation.
Excessive body fat gain, lipotoxicity, and type 2 diabetes
There are a few theories that implicate the interaction of abnormal fat metabolism with other factors (e.g., genetic factors) in the development of type 2 diabetes. Empirical evidence suggests that this is a reasonable direction of causality. One of these theories is the theory of lipotoxicity.
Several articles have discussed the theory of lipotoxicity. The article by Unger & Zhou (2001) is a widely cited one. The theory seems to be widely based on the comparative study of various genotypes found in rats. Nevertheless, there is mounting evidence suggesting that the underlying mechanisms may be similar in humans. In a nutshell, this theory proposes the following steps in the development of type 2 diabetes:
(1) Abnormal fat mass gain leads to an abnormal increase in fat-derived hormones, of which leptin is singled out by the theory. Some people seem to be more susceptible than others in this respect, with lower triggering thresholds of fat mass gain. (What leads to exaggerated fat mass gains? The theory does not go into much detail here, but empirical evidence from other studies suggests that major culprits are refined grains and seeds, as well as refined sugars; other major culprits seem to be trans fats, and vegetable oils rich in linoleic acid.)
(2) Resistance to fat-derived hormones sets in. Again, leptin resistance is singled out as the key here. (This is a bit simplistic. Other fat-derived hormones, like adiponectin, seem to clearly interact with leptin.) Since leptin regulates fatty acid metabolism, the theory argues, leptin resistance is hypothesized to impair fatty acid metabolism.
(3) Impaired fat metabolism causes fatty acids to “spill over” to tissues other than fat cells, and also causes an abnormal increase in a substance called ceramide in those tissues. These include tissues in the pancreas that house beta-cells, which secrete insulin. In short, body fat should be stored in fat cells (adipocytes), not outside them.
(4) Initially fatty acid “spill over” to beta-cells enlarges them and makes them become overactive, leading to excessive insulin production in response to carbohydrate-rich foods, and also to insulin resistance. This is the pre-diabetic phase where hypoglycemic episodes happen a few hours following the consumption of carbohydrate-rich foods. Once this stage is reached, several natural carbohydrate-rich foods also become a problem (e.g., potatoes and bananas), in addition to refined carbohydrate-rich foods.
(5) Abnormal levels of ceramide induce beta-cell apoptosis in the pancreas. This is essentially “death by suicide” of beta cells in the pancreas. What follows is full-blown type 2 diabetes. Insulin production is impaired, leading to very elevated blood glucose levels following the consumption of carbohydrate-rich foods, even if they are unprocessed.
It is widely known that type 2 diabetics have impaired glucose metabolism. What is not so widely known is that usually they also have impaired fatty acid metabolism. For example, consumption of the same fatty meal is likely to lead to significantly more elevated triglyceride levels in type 2 diabetics than non-diabetics, after several hours. This is consistent with the notion that leptin resistance precedes type 2 diabetes, and inconsistent with the “tired pancreas” theory.
Weak and strong points of the theory of lipotoxicity
A weakness of the theory of lipotoxicity is its strong lipophobic tone; at least in the articles that I have read. There is ample evidence that eating a lot of the ultra-demonized saturated fat, per se, is not what makes people obese or type 2 diabetic. Yet overconsumption of trans fats and vegetable oils rich in linoleic acid does seem to be linked with obesity and type 2 diabetes. (So does the consumption of refined grains and seeds, and refined sugars.) The theory of lipotoxicity does not seem to make these distinctions.
In defense of the theory of lipotoxicity, it does not argue that there cannot be thin diabetics. Many type 1 diabetics are thin. Type 2 diabetics can also be thin, although this is much less common. In certain individuals, the threshold of body fat gain that will precipitate lipotoxicity may be quite low. In others, the same amount of body fat gain (or more) may in fact increase their insulin sensitivity under certain circumstances – e.g., when growth hormone levels are abnormally low.
Autoimmune disorders, perhaps induced by environmental toxins, or toxins found in certain refined foods, may cause the immune system to attack the beta-cells in the pancreas. This may lead to type 1 diabetes if all beta cells are destroyed, or something that can easily be diagnosed as type 2 (or type 1.5) diabetes if only a portion of the cells are destroyed, in a way that does not involve lipotoxicity.
Nor does the theory of lipotoxicity predict that all those who become obese will develop type 2 diabetes. It only suggests that the probability will go up, particularly if other factors are present (e.g., genetic propensity). There are many people who are obese during most of their adult lives and never develop type 2 diabetes. On the other hand, some groups, like Hispanics, tend to develop type 2 diabetes more easily (often even before they reach the obese level). One only has to visit the South Texas region near the Rio Grande border to see this first hand.
What the theory proposes is a new way of understanding the development of type 2 diabetes; a way that seems to make more sense than the “tired pancreas” theory. The theory of lipitoxicity may not be entirely correct. For example, there may be other mechanisms associated with abnormal fat metabolism and consumption of Neolithic foods that cause beta-cell “suicide”, and that have nothing to do with lipotoxicity as proposed by the theory. (At least one fat-derived hormone, tumor necrosis factor-alpha, is associated with abnormal cell apoptosis when abnormally elevated. Levels of this hormone go up immediately after a meal rich in refined carbohydrates.) But the link that it proposes between obesity and type 2 diabetes seems to be right on target.
Implications and thoughts
Some implications and thoughts based on the discussion above are the following. Some are extrapolations based on the discussion in this post combined with those in other posts. At the time of this writing, there were hundreds of posts on this blog, in addition to many comments stemming from over 2.5 million page views. See under "Labels" at the bottom-right area of this blog for a summary of topics addressed. It is hard to ignore things that were brought to light in previous posts.
- Let us start with a big one: Avoiding natural carbohydrate-rich foods in the absence of compromised glucose metabolism is unnecessary. Those foods do not “tire” the pancreas significantly more than protein-rich foods do. While carbohydrates are not essential macronutrients, protein is. In the absence of carbohydrates, protein will be used by the body to produce glucose to supply the needs of the brain and red blood cells. Protein elicits an insulin response that is comparable to that of natural carbohydrate-rich foods on a gram-adjusted basis (but significantly lower than that of refined carbohydrate-rich foods, like doughnuts and bagels). Usually protein does not lead to a measurable glucose response because glucagon is secreted together with insulin in response to ingestion of protein, preventing hypoglycemia.
- Abnormal fat gain should be used as a general measure of one’s likelihood of being “headed south” in terms of health. The “fitness” level for men and women shown on the table in this post seem like good targets for body fat percentage. The problem here, of course, is that this is not as easy as it sounds. Attempts at getting lean can lead to poor nutrition and/or starvation. These may make matters worse in some cases, leading to hormonal imbalances and uncontrollable hunger, which will eventually lead to obesity. Poor nutrition may also depress the immune system, making one susceptible to a viral or bacterial infection that may end up leading to beta-cell destruction and diabetes. A better approach is to place emphasis on eating a variety of natural foods, which are nutritious and satiating, and avoiding refined ones, which are often addictive “empty calories”. Generally fat loss should be slow to be healthy and sustainable.
- Finally, if glucose metabolism is compromised, one should avoid any foods in quantities that cause an abnormally elevated glucose or insulin response. All one needs is an inexpensive glucose meter to find out what those foods are. The following are indications of abnormally elevated glucose and insulin responses, respectively: an abnormally high glucose level 1 hour after a meal (postprandial hyperglycemia); and an abnormally low glucose level 2 to 4 hours after a meal (reactive hypoglycemia). What is abnormally high or low? Take a look at the peaks and troughs shown on the graph in this post; they should give you an idea. Some insulin resistant people using glucose meters will probably realize that they can still eat several natural carbohydrate-rich foods, but in small quantities, because those foods usually have a low glycemic load (even if their glycemic index is high).
Lucy was a vegetarian and Sapiens an omnivore. We apparently have not evolved to be pure carnivores, even though we can be if the circumstances require. But we absolutely have not evolved to eat many of the refined and industrialized foods available today, not even the ones marketed as “healthy”. Those foods do not make our pancreas “tired”. Among other things, they “mess up” fat metabolism, which may lead to type 2 diabetes through a complex process involving hormones secreted by body fat.
References
Humboldt, A.V. (1995). Personal narrative of a journey to the equinoctial regions of the new continent. New York, NY: Penguin Books.
Unger, R.H., & Zhou, Y.-T. (2001). Lipotoxicity of beta-cells in obesity and in other causes of fatty acid spillover. Diabetes, 50(1), S118-S121.

51 comments:
"Avoiding natural carbohydrate-rich foods in the absence of compromised glucose metabolism is unnecessary."
thank you. i'm off to eat my sweet potato now.
Is leptin the only hormone secreted by fat cells?
Fiber products are often labeled healthy.. but would these also be considered refined? Have humans evolved to eat whole grain wheat or could this also be responsible in part for messing up fat metabolism?
Also, if blood level > 165mg/dl after eating, or having a steady state above 115 mg/dl are bad indicators, what are ideal numbers?
Seems like the preferred carbohydrate sources should also be high in fiber.
Dr. Lustig on the importance of fiber:
http://www.youtube.com/watch?v=dBnniua6-oM#t=1h12m53s
The Kitavanian diet is probably very high in fiber.
Dr. Lustig interview by Jimmy Moore:
http://tinyurl.com/2e2u2b9
Lustig doesn't particularly care for low-carb per se as he's much more in favor of high fiber.
Looks like Lucy may have been a meat eater after all. I first read about it in this blog post.
http://ecodevoevo.blogspot.com/2010/08/ten-scratches-on-two-bone-fragments.html
Here's a link to the Nature abstract.
http://www.nature.com/nature/journal/v466/n7308/full/nature09248.html
Hi bee.
Enjoy your sweet potato. That's one of the staple foods of the traditional Okinawan diet.
Hi js290.
Fiber feeds our gut bacteria. The byproducts are supposed to be health-promoting, even though there are widely divergent opinions on the subject. Fiber certainly seems good in the context of the SAD diet.
Still, the Inuit consume very little fiber, and there is no diabetes among them. They are practically free from the diseases of civilization when they stick to their traditional diet.
Hi Anon.
One cannot go very wrong consuming only (or almost only) plant products that can be eaten raw. Staying away from wheat products is probably a good idea.
A rule of thumb that I follow is to avoid foods in quantities that cause my blood sugar to spike higher than 140 mg/dl anytime after a meal. Having said that, it takes a lot of high glyc. carbs to make that happen.
Thanks Karin.
So Lucy liked a bit of meat; makes sense, given that chimps also do. Maybe they'll find the same thing about Ardy.
Still, Lucy's GI tract and teeth suggest a primarily vegetarian diet. And certainly we have several adaptations that help with fruit-eating. Fructose from fruits seems to help with glycogen replenishment:
http://healthcorrelator.blogspot.com/2010/06/fructose-in-fruits-is-good-for-you.html
I wonder how much of a role epigenetics plays in what cultures are able to healthily eat?
Hi js290.
Can you elaborate on that?
I don't know if you've seen this post:
http://healthcorrelator.blogspot.com/2010/01/how-long-does-it-take-for-food-related.html
There may be genetic differences among isolated populations, due to evolution of traits in response to the availability of certain foods and not of others.
Hi Ned,
What do you think about the idea that hepatic insulin resistance is the core driver of the metabolic syndrome?
As I understand it, hepatic insulin resistance has been linked to excessive fructose triggering the JNK-signaling pathway and hepatic inflammation caused by excess omega 6 and/or endotoxins.
The end result is escalating hyperinsulinemia and hyperglycemia as the liver enters a state of constant gluconeogenesis. This condition is also accompanied by de novo lipogenesis and both peripheral and ectopic fat deposition.
(Hyperlipid @ http://high-fat-nutrition.blogspot.com/ is a good source about this perspective.)
This "liver-centric" model doesn't contradict the idea that lipotoxicity is what kills the pancreas, but it suggests that obesity is more of a symptom than a core cause in the metabolic syndrome and type 2 diabetes.
Hi Christian.
I guess the problem with that idea is that excessive fructose will be converted into fat by the liver and secreted in VLDL particles. The body does not simply get right of that fat if it is not needed. It eventually gets stored as unnecessary body fat, and then you have the precondition for lipotoxicity.
Moreover, that excessive fructose is often associated with a fatty liver. That is not a good thing because body fat should be stored in adipocytes. And this is exactly what the lipotoxicity theory predicts. That is, the body fat “spill over” effect, where fat is stored where it shouldn’t be. That “spill over” effect leads to abnormal liver function.
Hi Ned,
Re fructose and it's link to the metabolic syndrome, the theory is that there is a more direct connection between fructose metabolism and hepatic insulin resistance than through fatty liver and/or de novo lipogenesis.
The mechanism is outlined beginning on page 32 in this PDF.
http://www.cce.csus.edu/conferences/childobesity/09/docs/handouts_r3/How%20Sweet%20It%20Is%20-%20Addiction,%20Reward%20and%20Childhood%20Obesity_b.pdf
The key section is:
"Intrahepatic lipid and FIP [Note: FlP is a direct metabolite from fructose] are both able to induce the transcription of JNK-1 (45), which induces serine phosphorylation of insulin receptor substrate-1 (IRS-1) in the liver (47), thereby preventing normal insulin-stimulated tyrosine phosphorylation of IRS-1, and promoting hepatic insulin resistance. This will prevent Foxo1 from becoming phosphorylated; Foxo1 enters the nucleus and gluconeogenesis ensues, raising blood sugar and furthering the hyperinsulinemia (43). "
This is not to contradict the idea that lipotoxicity is ultimately what produces the end state of type 2 diabetes, but it's relevant to a discussion of the bad things (hyperglycemia, hyperinsulinemia, high blood pressure, and others) that happen on the road there.
A very important post. This should be required reading for those who insist that a low-carb diet is necessary to prevent type 2 diabetes.
The lipotoxicity theory makes sense to me and matches my clinical and personal experience. For example, I have no blood sugar regulation problems at all. I can eat a potato or large portion of other unrefined carbohydrate and my blood sugar is still well within normal limits 1- and 2-hours after a meal.
However, some of my patients would see their blood sugar skyrocket up to 180 or more with similar meals. The theory described in this post provides - in my mind, at least - the most plausible explanation for this discrepancy. There is nothing wrong with my fat metabolism; thus, I can tolerate the carbs. But my patients with abnormal fat metabolism and consequent insulin and leptin resistance cannot.
The one area I'd like to understand better is what would cause the threshold of body fat gain that precedes lipotoxicity to be so low in some people. I have one patient who is very lean, yet has clear signs of leptin and insulin resistance and lipotoxicity. What could cause this? My guess is that either adrenal over- or under-activity and/or thyroid hypofunction are involved with the "lean diabetic" type.
High or low cortisol due to adrenal stress causes dysglycemia - independently of weight gain, lipotoxicity and insulin/leptin resistance.
Low thyroid function slows the rate of glucose uptake in the blood, decreases the rate of glucose absorption in the gut, slows the response of insulin to blood sugar, and slows the rate of insulin clearance from the blood.
Finally, I suspect that some of what we refer to as garden variety type 2 diabetes is actually autoimmune mediated (see this paper: http://endo.endojournals.org/cgi/content/full/146/10/4189). For example, it's not uncommon for Hashimoto's patients to also produce antibodies to GAD. But even a systemic inflammatory response could decrease insulin and leptin receptor site sensitivity without necessarily causing weight gain.
Hey Ned, thanks for the shout out and your post on my blog. This is complicated stuff. I read Unger but I also read this.
Lack of Lipotoxicity Effect on β-Cell Dysfunction in Ketosis-Prone Type 2 Diabetes.http://care.diabetesjournals.org/content/33/3/626.long
I don't think we can get around Lipotoxicity. It seems to be an obvious problem. The "what, where and when" of its effects is the big question.
I am not a big fan of "tired pancreas" mainly because KPD's are infamous for losing beta cell function in a high glucose environment and regaining beta cell function when the glucose is lowered. Of course, this is a broken metabolism. This sticks out because part of a regulatory mechanism is missing. I just have to believe that there are some other things going on in beta cell function and glucose levels that we are missing.
More to come, still mulling.
Hi Christian.
We have to keep an open mind. But the claim that fructose induces hyperglycemia right away, by stimulating gluconeogenesis, conflicts with a lot of evidence. More specifically, it conflicts with evidence showing that fructose by itself has essentially no effect on blood glucose levels. See the link below for one of the many studies that show that; an old and widely cited one.
http://www.ncbi.nlm.nih.gov/pubmed/2394949
Now, when you have a lot of fructose and glucose consumed at once in easily digestible form, as in a regular soda, then you have a problem. The liver is overloaded, and gives precedence to fructose. So it does not grab the glucose right away as it should.
Blood glucose then rises abnormally. This is essentially a temporary form of liver insulin resistance. One of the main effects is that more glucose is picked up by fat cells (via GLUT4) than should have been the case. Another effect is that you also have higher than normal blood glucose levels, and thus more glycation.
By the way, I don’t know if you have seen this post (link below), which essentially says (based on a study with rats) that fructose and glucose from fruits seems to be a better fuel mix for glycogenesis than glucose alone. It also talks about some of Lustig’s claims and a discussion on Alan Aragon’s blog.
http://healthcorrelator.blogspot.com/2010/06/fructose-in-fruits-is-good-for-you.html
Hi Chris, thanks.
Yes, quite a few possibilities for the threshold. Add growth hormone to that list; sometimes it being low leads to high insulin sensitivity:
http://healthcorrelator.blogspot.com/2010/08/growth-hormone-insulin-resistance-body.html
I think you are right about people often being misdiagnosed as type 2.
Hi Michael, you're welcome.
Unger doesn't seem to be helping his case by blaming dietary fat. Among his audience (actual and potential) there are a lot of low carbers who swear by their high-fat diets.
Thanks, Ned. I've heard Dr. Schwarzbein talk about the importance of GH, and it seems to have a variety of effects when it comes to blood sugar regulation.
At this point Dr. S is much more focused on reducing stress and other factors that influence what she calls the anti-insulin hormones (cortisol, epinephrine, norepinephrine, glucagon and possibly GH) than she is on regulating insulin directly. I'm sympathetic to this approach. Stress (of any kind - emotional, psychological, physiological) will elevate these hormones, and all of them oppose insulin, thus leading to chronic dysglycemia.
Add the influence of autoimmunity and inflammation, both of which are often overlooked in the conventional model, and you've got a compelling explanation for how diabetes can develop without even talking about carbohydrate intake (except refined carbs, which contribute to inflammation, stress and autoimmunity).
Hi Ned,
There is no claim that fructose induces hyperglycemia right away. The causation as I understand it is between excessive fructose (consumption beyond filling liver glycogen) and a sustained state of liver insulin resistance and accompanied gluconeogenesis.
Perhaps the keyword is "sustained", and that steatosis, ie a form of lipotoxicity, is what it takes to have a chronically insulin-resistant liver.
In either case, I think that the main point is that hepatic injury seems to be at the center of the metabolic syndrome, and thus needs to be part of a model as a distinct feature. (No hepatic injury; no type 2 diabetes is my mental picture for now.)
Aside from fructose, hepatic injury seems also to be a possibility from oxidative stress from excess PUFA as well as endotoxins carried in by gluten, so the link to neolithic foods is there in a way that makes sense given the liver's role as a gatekeeper.
A related point is that the hepatic insult seems to be mitigated in individuals whose bodies are prone to store fat in adipocytes and thus would gain some anti-inflammatory and insulin-sensitizing protection from adiponectin. This would help explain why thin persons with the metabolic syndrome often have more severe metabolic dysregulation than mildly obese persons. (This is the point about protective obesity that Unger has talked about lately.)
BTW, I'm not trying to debate you here. I'm interested in integrating the most compelling pieces that I find into a coherent picture. Your thoughts are among those very compelling pieces.
Ned,
thanks for pointing me to your other post. Does your analysis assumes that the expression of the genes remain constant throughout one organism's life? Epigenetics seem to show that the expression could be different even among people with identical genes. So it may not be necessary to wait for a mutation.
http://www.nytimes.com/2008/03/11/health/11real.html?_r=1
http://www.marksdailyapple.com/control-gene-expression/
The biochemistry has to work the same for everyone. But, then how those biochemical reactions get expressed may vary. Would Otto and Ewald's sensitivity to insulin differ given their different physiques?
It's conceivable that rituals and customs that make up a culture help set the epigentic factors that has allowed it to survive.
This epigenetics thing is all new to me, and I'm certainly not studying it at any in depth level, so all I can really do is ask dumb questions about it. :-)
Just a layman here, not sure why the distinction between fructose and glucose.. aren't the differences pretty minor (i.e. sucrose = fructose + glucose)? And early in digestion everything goes to glucose anyways?
But if I understand this article/comments correctly, excess fructose in the blood gets stored as fat in the liver, and this MAY cause metabolic and/or pancreatic issues.
Anonymous layman:
http://www.youtube.com/watch?v=dBnniua6-oM#t=42m57s
http://www.youtube.com/view_play_list?p=86C665F9EC5C4B7F
Hi Christian.
Thanks for the clarification. There is no problem with debate; that's how we learn. I'll have to look more into that.
Just to add something into the mix: I suspect that many of the thin folks who develop the metabolic syndrome (which are a minority, as a group) are thin because of stress-induced problems.
As such, they often have low BMI but a relatively high body fat percentage. Also, stress-induced abnormal cortisol secretion leads to the accumulation of visceral fat, even if subcutaneous fat is relatively low.
Still a working hypothesis though.
Not to mention that chronic stress:
- decreases receptor site sensitivity
- decreases proteonomic response
- causes inflammation of the hypothalamus
- causes chronic dysglycemia
- causes systemic inflammation
all of which contribute to metabolic syndrome.
Hi js290.
Practically all phenotypic traits (e.g., body fat percentage) that have a genetic basis are the result of gene-environment interactions. The exceptions are very few - e.g., blood type.
So let's say we have two identical twins A and B, both with genotypes that protect them against the metabolic syndrome. If B's development is slightly different (in a way that is relevant for MB), then B may have a higher or lower chance of developing the MB than A.
The thing is that, even in twins raised together, there are always differences in environmental and developmental factors. Depending on the phenotypic trait, small differences can be greatly amplified by the body's responses.
This reminds me of a case of a co-worker who recently died of an autoimmune disease (lupus). His identical twin is healthy, and has never had any sign of lupus.
Thanks Chris.
Indeed, stress is more of a problem than many people think. Especially when stress is not accompanied by the violent muscle contractions that are supposed to follow it (the fight-or-flight response).
Hi Anon.
Based on the theory of lipotoxicity, and the evidence used to support it, it seems that excess fructose leads to abnormal secretion of small VLDL particles. Those particles deliver their cargo (mostly fat, but also cholesterol) to body fat cells and other tissues (e.g., muscle).
So excess fructose probably makes you fat first, over time leading to a fatty liver, as proposed by the theory of lipotoxicity. But this is a point of debate. Certainly there is evidence that this happens, but in some people (or maybe a lot of people) chronic excess fructose leads to liver injury, as Christian pointed out.
Now, fructose from fruits seems to be harmless, a point that is made by Lustig himself. So the problem seems be primarily with things like man-made foods with high fructose corn syrup added.
Since we are talking about VLDL particles, here is a post with a photo of these and other particles:
http://healthcorrelator.blogspot.com/2010/02/large-ldl-and-small-hdl-particles-best.html
Ned, seems like the metabolism of fructose would be the same regardless of the source. The difference seems to be that fruit probably have less fructose content compared to soda or juice and has fiber and beneficial micronutrients.
The problem with fructose is apparently chronic rather than acute. The fact that HFCS is in everything makes it a chronic problem for just about everyone. This is especially bad since fructose is metabolized only by the liver.
Hi js290.
I think that something about getting fructose in liquid form is particularly bad, but I don't have a reference for that. It certainly isn't natural.
Fructose is not only metabolized by the liver, although most of it is under normal circumstances:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1136029/
Among other things, fructose is a good fuel for glycogenesis in muscle tissue (as well as liver).
Ned, perhaps another way to look at it is fructose without fiber is not natural?
Also, as you point out in your other post, glycogenesis requires glycogen depletion. Most people don't ever get to the point of being glycogen depleted. It seems like to get to that state, one has to do something steady state for a very long time, like run a marathon. Or, do high intensity interval training, like Tabata intervals at 170% VO2max. Or, high intensity strength training to failure.
Without the glycogen stores drained, there may not be much benefit in the fructose boost to glycogenesis.
Severe muscle glycogen depletion can happen with exercise, but our liver glycogen tank goes up and down all the time. Liver glycogen is used by our body to maintain blood glucose levels within a certain range.
For example, after a night of sleep our liver glycogen is a bit low. If you eat one fruit or two in the morning, it goes up a bit.
It seems that man made processing / sterilising of food is one of the root causes of all these diseases of civilisation, Fructose being no exception.
I think physical inactivity is a big contributor to diabetes and certainly confounds a poor diet. I noticed I became alot more carb tolerant since going to a gym. ( And consequently became more carb intolerant when I stopped cycling to work. )
With regards to the glycogen/fructose issue, it seems that muscle glycogen is mainly used by type IIa muscle fibres which would suggest that if the exercise intensity is not at the right level you wont deplete it.
Are there any studies on atheletes consuming HFCS and the consequences? That would be interesting.
Hi Kindke.
The studies that I've seen are mostly short-term. I think that athletes tend to suffer the least from consumption of HFCS drinks (and similar drinks), because of their glycogen depletion levels. Glycogen synthase activity will be very high in depleted muscles. This will lead to glycogenesis in muscle directly from circulating fructose and glucose, lessening the burden on the liver.
I am not sure glycogen depletion is more accentuated in fast-twitch fibers. I've seen some photos of leg muscle glycogen depletion in endurance athletes - marathon runners. It is major, especially after competition, and very localized.
Kindke, IIa fibers are intermediate and can apparently use both aerobic and anaerobic metabolism. The slow twitch (type I) fibers are largely aerobic.
Ned, my guess is marathon runners use primarily use type I and IIa fibers, until the end when they're sprinting for the finish. Type IIb fibers are anaerobic, meaning they can burn the glycogen stored in them and can't efficiently use oxygen as fuel. It seems like muscle fiber type can change depending on training, too.
Here's a youtube video of McGuff talking about adrenalin, hormone sensitive lipase, and glycogen:
http://www.youtube.com/watch?v=ToGt_GYCUmY#t=2m53s
Hi. Yanno, I've always been very skeptical of the "worn-out beta cells" idea just because that generally isn't how our body operates. We don't get worn-out muscle cells or worn-our fat cells; instead, we get proliferation.
The lipotoxicity hypothesis is interesting. But for my part, I always assumed that what seemed to be beta-cell burnout was just the final stage of insulin resistance. If you get to the point where there are huge quantities of glucose and insulin circulating round the clock, the body can't do too much about the glucose, but it might be able to at least send some sort of message shutting down insulin output.
Optimal? No. But if the glucose levles are no longer substantially affected by the presence of high levels of insulin, then you have all the negative effects of high insulin without any regulatory benefits. So it seems to me to make sense at that point to tell the beta cells to shut down production...
Hi David.
Yes, the pancreas getting tired is definitely not the way the body operates. If that was the case, a lot of hormone secretion organs would get tired over time, and we would lose the ability to produce glucagon, cortisol, adrenaline, leptin etc.
Your hypothesis is interesting though - shutting down insulin production being a compensatory adaptation. The lipotoxicity theory has an upper hand over it at the moment because it is consistent with the apoptosis process started with abnormal fat metabolism.
i keep being brought bac to this post trying to uderstand the liotoxicity theory...
it essentially makes taubes wrong, does it not? i am starting to agree with it, that excess food of an unnatural nature, be it carbs/fat/protein is the reason fat spills over due to a lackof needed vitamins/minerals that faled to be present in the unnatural food consumed. without the needed nutrients, but with an excess of food, your body has no choice but to store fat
so essentially, one can use a HIGH fat diet, with necessary protein/carbs to lose weight once damaged and thus promote insulin sensitivty through IF/lifting/weight loss. but once that occurs, shouldnt the body be prime to use NATURAL carbs for the better?
i think maybe the problem starts at weaning though, passing on bad genes from a previously bad diet, not breastfeeding, and resulting in a bad gut flora. this person then is prime to have metabolic problems, and nutrient absorbing difficulties. the healthy baby though should have no problem eating anything they want in regrds to real food. their body sould naturally get hungry/fed. the unhealthy baby will never be full, always thinking about food, and gaining fat b/c of excess unntural food.
the lipotoxicity theory makes a lot more sense to me than taubes ever did. also should follow from the theory maybe should be to stop 'blaming' contets of real food, like omega 6 in nuts and avocados b/c theres a world of difference between that O6 and that found in vegetable oil. same with fructose in fruits vs a soda
i guess i dont really have a question just if you have any further information on this theory i would be very interested
Hi Mal.
Taubes talks about a lot of things, and leaves the door open for conclusions. I think GCBC is mostly a book about how science can go wrong, as opposed to a book that proposes a new theory about health.
Having said that, the theory of lipotoxicity is inconsistent with the notion that a high carb diet will necessarily lead to obesity and T2D. And many people associate this notion with Taubes, because Taubes does hint at that.
One of the main practical applications of the theory of lipotoxicity is that a good body composition (a reasonable amount of lean body mass, with a low body fat percentage) is a good shield against the metabolic syndrome and T2D. And one can achieve that eating plenty of natural carbs, as long as one is not insulin resistant.
I realize the last post was back in 2010, so hopefully the previous contributors will pick this up and respond.
What do you all think about the following?
I saw a "Discovery channel" documentary and the study showed that:
• RNA messengers come from artery walls and tell stem cells in the pancreas to "become" beta cells
• These RNA messengers fail to communicate (with the stem cells) when the arteries in and around the pancreas become sufficiently separated from the organ (such separation resulting from increased fat—I postulate)
• This results in an inadequate production of beta cells.
• This results in deficient beta cells and an inadequate supply of insulin.
The program never suggested why the artery gets separated just that when it does or did, the RNA messenger failed to communicate with the stem cells. I postulate the separation is a result of fat moving the artery too far away. The separation tolerance is very minimal… we are talking a millimeter or even microns here. So even a little bit of separation can cause the communication to fail. Once failure occurs, stems cells do not know they need to become beta cells, and beta cell production is decreased. Some not separated arteries will continue sending messages for the need for beta cells, but none-the-less, there are inadequate requests, and beta cells simply do not get produced in sufficient supply to keep up with insulin production requirements. All, possibly because of the fat which moves the artery too far away. Once Insulin production is inadequate, high blood sugar sets in, of course.
The program explained that the RNA messenger comes from the wall of arteries; that such messengers are responsible for telling stem cells "Hey, you need to become a Beta cell."
The concept goes, that without Beta cells being replenished, they don't get tired per se, they simply fall behind as there is not enough to do the job where before sufficient quantities of them were able to keep up with insulin demands.
I found this particularly interesting and conceivably explicable as to what happened to me:
I was 235 lbs, never diagnosed with Type 2. Had all the symptoms, but did not know such symptoms were related to diabetes. I was 40. I had tingling feet, blurred vision, sores slow to heal, was irritable, tired all the time, itchy like crazy and a big gut. Well, I wanting to be more healthy, so I went on a stir-fry diet (home prepared), eliminated dairy, ate a very limited diet as follows (oh, and by the way, I discarded everything that was sold or came in a package, bottle, tub, jar or carton (except for applesauce, peaches, eggs, oil, almonds, molasses, raw honey, maui sauce, baking soda & baking powder, yeast, spices and salt). Sea salt was used.
BREAKFAST:
• Cooked Whole Oats
• Extra-virgin Olive Oil
• Raw Honey
• Peaches (peaches were canned, but in a light syrup)
• Salt
OR
• 100% Whole Wheat Pancakes (home prepared from whole grain ground seed in a blender)
• Extra-virgin Olive Oil
• Egg
• Baking Powder
• Salt
• Topped with Applesauce (this was the no sugar added, canned version)
OR
• Fried Eggs
• Extra-virgin Olive Oil
• Fresh grated potatoes (hash browns)
• Seasonings
• Salt
LUNCH
• Romaine Lettuce
• Fresh Carrots
• Fresh Tomatoes
• Raw Almonds
• Extra-virgin Olive Oil
• Spices
• 100% Home Made Bread (Ground Whole Wheat Seed, Water, Extra-virgin Olive Oil, Water, Honey, Molasses, Yeast and Salt)
• Raw Honey (on the bread)
DINNER
• Stir Fry (home made) with
• Fresh Broccoli
• Fresh Onions
• Fresh Carrots
• Raw Almonds
• Canned Bamboo Shoots
• Canned Water Chestnuts
• Maui Sauce
• Occasionally brown rice was also cooked and eaten with the stir fry, but usually it was just the half cooked stir fried veggies.
• 100% Home Made Bread (list of ingredients as shown above)
• Raw Honey (on bread)
(continued on next post)
(Continued from previous post)
Perhaps because of low levels of activity Syndrome X begins, and activity levels decrease and fat accumulates. But once fat sets in and insulin production goes down (insufficient beta cells), you simply don’t have the energy to even want to do activity. So, I think it starts with lower activity and continual intake of high calorie foods (HFCS) which then results in getting fat, which then results in inadequate RNA messengers communicating the signal to produce more beta cells. I think that the ACTUAL REASON insulin production decreases and ultimately when reversed Type 2 diabetes can be reversed also.
The cause is FAT collecting between the arteries near or in the Pancreas. Get rid of that fat, and you can solve the insulin deficiency issue. Of course the liver must also be fat decreased so it can work at its best as well.
The underlying cause is eating things that make you fat—too much and not the right things. Also, as you get fat, and insulin supplies go down, the desire to even do activity is decreased because you just don’t feel like doing anything. Once (before diagnosed) I lost the weight, even though I was 40, I felt like a kid and HAD the energy to do all sorts of things, including spring off the sofa which was not even necessary, but so easy to do. Why? I had the energy and the attitude to do it. I was not taking insulin. I was not over weight, I was not yet diagnosed, and I was a 40 year old man with the extremely high libido (which only months before was non-existent) and (now) energy to leap off the sofa and for no good reason.
C) Heat (sauna) increases uptake of insulin. (No wonder one feels good, especially if one is diabetic after they come out of the sauna.) For sure circulation is improved, an aerobic state (while in the sauna) is created, toxins are sweated through the pores along with water, insulin uptake is increased, blood sugar goes down—all while just sitting there doing nothing. You may be doing nothing, but your body thinks it’s on a treadmill as you heart is working just the same as if it was. So any idea that a sauna just sweats water weight, well that is clearly wrong. A sauna causes aerobic activity just the same as a treadmill. The toxins lost help the body to drop “fat”. Fat is held when bodily toxins are high. Lower toxins, and fat is no longer needed. Lower fat and well, insulin usage and production improves (as long as the fat is also lost in the artery areas that are separated and blocking the RNA signals. If the fat is not lost there, then your doctors tells you, “Your beta cells are all burned out.” Not even. Just missing, but not burned out.
D) As more beta cells are grown, insulin production increases. This is nothing new. And so, if not, why is not the question being asked, “Why are the beta cells not reproducing?”
Look at it from my observational stand point:
1) After losing weight…
2) No diabetic symptoms.
3) Endless energy.
4) No need for insulin or knowledge there was even a problem--which altogether vanished.
5) Return to being obese, all problems return.
6) Go on insulin--and now weight loss is impossible. Why? I think I am in a state of constant hyperinsulinemia. Duh!
7) Go off my insulin (which I did), eat only raw food (which I did), exercise, do sauna, etc. (which I did--this was all after being diagnosed with Type 2), and my A1C went from 13 to 6.8, and I was told I was now a mild diabetic. Still overweight, 195 and still insulin dependent.
(continued on next post)
(Continued from previous post)
Now I can see the obvious difference in insulin production at 195 lbs v.s. 170. Before there was not sufficient, now there is so much more. I expect that when I get down to 170, no insulin injections will be needed.
They say there is no cure for diabetes. Of course, there isn’t. If you store fat between your ateries and the beta cells (genetically speaking), and you get fat again, you will have the process begin all over again. So, factually, there is no cure until you are able to stop (change you genes) storing fat how you store it. Want to not have the problems? Don’t get fat. Not exactly a cure, but certainly a means of preventing the vicious cycle.
Doctors tells me, don't ever go off your insulin. Well, personally, I feel like the insulin keeps one perpetually fat, hence very unhealthy, hence the chances of the RNA messengers ever reaching the target are diminished if not eliminated altogether. Now, one may say, “What about fat people who don’t have diabetes?”
And I’d say, they don’t have “separation” or malfunction of RNA communications. In other words, their genetics don’t store fat between the arteries and/or separation does not occur. They may be a fat toad, but the fat storage is not in and around or between the arteries and beta cells continue to be reproduced in sufficient supply.
Clearly before manufactured insulin was available, the treatment was no food.
Why not, instead:
1) Use insulin sparingly (when needed) to keep glucose in a healthy range.
2) Then, change one's diet to only raw veggies for a month or two
3) Eat less in general
4) Increase activity and exercise more while detoxifying daily in the sauna
5) This will reduce insulin needs to none –eventually (i.e. no supplemental insulin injections)
6) Continue to eat raw and exercise daily (aerobically speaking)
7) Lose the fat
8) Re-establish the RNA communication with the stem cells in the pancreas that originate from the arteries
9) Through restored RNA messenger communication, the stem cells will produce beta cells
10) Hence, naturally Increase beta cell production
11) Hence naturally increase beta cell count
12) Hence naturally increase insulin production through more beta cell count
13) Finally, solve the inherent problem by NEVER going back to what clearly contributes to being fat (no exercise, HFCS, processed foods way too high in calories and way too low in fiber, and nutritionally dead to begin with—i.e. SAD foods
14) Now, that the body has a chance to do its job--the job its been doing for 40 years just fine, until the metabolism changed significantly due to inactivity, due to lack of energy sufficient to even have adequate activity, due to accumulating fat, due to artery separation, due to lack of beta cells being produced resulting in deficient insulin, which caused the high glucose levels in the first place which resulted in all the symptoms.
It appears to me that this explains “diabetes”. I am sure there is more to it (fatty liver, etc.) but this seems to be at least one of the major underlying problems: “RNA Disconnect—Beta Cell Production Shut Down”
What do you think? Can you shed some additional light on this subject? I am interested in knowing as much as I can about this subject as I did what I did, unknowingly, and it produced what it produced. Now I have the diagnosis, and I am going to go back to “thin”. I think it will repeat what happened before, and I would like to know as much as I can about this “thing”.
This post is a revised version of a previous post. The original comments are preserved here. More comments welcome, but no spam please!
Great post, especially the part about avoiding carbs in a traditional diet context being unnecessary. (High-carb diets tend to be less nourishing, so present the problem of malnutrition, but this does not lead to diabetes.)
Two studies I cam across recently that shed some light on incidence of diabetes in a modern-diet context:
"The Natural PPAR Agonist Linoleic Acid Stimulated Insulin Release in the Rat Pancreas"
https://www.researchgate.net/publication/247157499_The_Natural_PPAR_Agonist_Linoleic_Acid_Stimulated_Insulin_Release_in_the_Rat_Pancreas
and
"Human high-density lipoprotein particles prevent activation of the JNK pathway induced by human oxidised low-density lipoprotein particles in pancreatic beta cells"
https://link.springer.com/article/10.1007/s00125-007-0642-z
From my readings, a necessary ingredient for a high-carb diet to induce diabetes is a significant omega-6 intake. The first paper injected LA, but if this same process occurs via the diet, that could explain hyperinsulinemia which itself induces insulin resistance.
At the back end, oxidized LDL is produced from dietary n-6 intake (markers are all products of N-6 peroxidation).
Damage to beta cells via oxLDL is, to me, a better explanation for reduced function than "tiredness".
OxLDL also induces an autoimmune response, as the body has mechanisms to clear it, which appear to be overwhelmed at high levels of N-6 intake (along sith several other compensatory mechanisms).
Dang, Ned, way to revive and oldie but a goodie. :-)
In the previous comments about fiber and gut bacteria, looks like gut bacteria converts the fiber to butyrate.
Impairment of fat metabolism is still largely insulin driven. Insulin's first order effect is to inhibit lipolysis to prevent instant death from ketoacidosis, see T1DM. And, according to the Randle hypothesis, we can use glucose or fat, but not both at the same time.
While glucose measurement is useful, it's not a good proxy for insulin response. My unqualified speculation is that blood ketone levels may be a better proxy for insulin.
A couple years ago, Unger proposed a central role for glucagon in diabetes. This theory still involves lipotoxicity, which produces the intracellular toxic compound ceramide. For more info:
https://diabeticmediterraneandiet.com/2015/01/10/dr-roger-unger-and-his-glucagon-centric-diabetes-model/
-Steve
Hi Ned,
Can you provide any guidance on how to compare foods using a glucose meter e.g. should the carb/calorie content or portion size be kept constant and what about protein? and do you think testing at +1 and +3 hours (middle of reactive hyperglycemia range) is sufficient.
Additionally, are you aware of any foods that show large individual variation?
I’d recommend taking blood glucose measurements in 15-minite intervals, starting 15 minutes after the meal and ending after blood glucose stabilization. Meals with carbs. should be the target. Meals with protein and no carbs. are interesting to check as well, as they are likely to lead to a small reduction in blood glucose – due to the interplay of insulin and glucagon.
This post is a revised version of a previous post. The original comments are preserved here. More comments welcome, but no spam please!
Post a Comment